We show you step by step what to expect when you visit the CTAFC: from your first visit to the day of your procedure as well as post-op.
Step 1. Meet our team
The first team members you wil encounter, will be our team at reception:




One or more of these ladies will assist you with any administrative or medical aid querries, follow-up consultations, obtaining your records and more.
Step 2. Your consultation with our clinical technologists
During your first visit, you will probably first be in the good hands of one of our two clinical technologist. Ryan or Karl will test your heart rate with an exercise EKG and will also perform a sonar of your heart. The cardiologists need the results of these tests before they consult with the patient.
Learn more about the tests to diagnose your arrhythmia.
Our clinical technologists are Ryan and Carl:


Step 3. Your consultation with the medical specialists
With the results of the heart tests at their disposal, Dr Razeen Gopal, one of just a handful cardiologists in South Africa with complete and international training in electrophysiology and the most accomplished electrophysiologist in the Developing World (outside the USA , Europe and Britain) or Dr Sumanth Karamchand, cardiologist and a fellow in electrophysiology, will consult with you, and discuss your diagnosis and treatment options with you. They will suggest the best treatment option. You will make the final decision.

Step 4. If you have chosen the catheter ablation option, then you are heading to theater
The morning of your ablation a CT or MRI of your left atrium is performed so that we can import this into our EP Systems.
The electrophysiology theater is on the second floor of the Heart Unit at Mediclinic Panorama. The theater is state of the art and equipped with the latest technology needed to perform any procedure to treat a slow, fast or irregular heart rhythm.
Before you go to theater, or even sooner, you’ll meet our dedicated arrhythmia nurse, Sr Melinda Schutte, who will keep a watchfull eye on you after your surgery when you are in ICU.

Look at this video inside the theater:
One of two dedicated anaesthetist will take care of you in theater. They are:


A number of techniques and approaches are currently used.
For atrial fibrillation patients: The patient is often in atrial fibrillation at the beginning of the procedure.
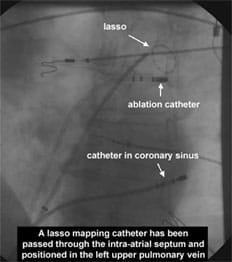
We also confirm that electrical isolation has been achieved by using a pulmonary vein mapping catheter. Alternatively the electrical isolation of the veins may also be achieved by a technique called electroporation or by Cryo ablation. Once this has been completed the patient will hopefully have returned to sinus rhythm. If they haven’t then we perform an external cardioversion with standard defibrilation pads.
The success of the procedure does not seem to be predicted by whether the patient returns to sinus rhythm with the cardioversion or with the ablation. Following the left atrial procedure for atrial fibrillation ablation, we also perform an ablation of the isthmus between the tricuspid annulus and inferior vena cava which will also prevent atrial flutter occurring after the procedure.
The team in theater to assist Drs Gopal and Karamchand are:





Post-op
After all procedures an echocardiogram is performed to make sure that fluid has not leaked out of the heart.
The patient is then returned to the ward for close monitoring by the nursing staff. Once the heparin (blood thinning medication) has worn off the sheaths (fine tubes) in the groin can then be removed.
After this another 2-3 hours of flat bed rest is required while the veins start to heal up and a little longer before the patient can get up and walk around.
Even if the patient was not on anti-coagulant therapy before the procedure, warfarin will be re-started on the day of the procedure with the heparin being re-started the next day. The heparin will be continued until the anti-coagulant has taken full effect which is usually about 4 days.
It is not unusual to have symptoms of chest pain and palpitation after the procedure. Even if atrial rhythm problems occur these, can often resolve on their own after 3 to 6 months. We are not sure why this happens but it seems likely that inflammation of the atrium following the ablation can be one of the reasons.